mast cell tumorS
BACKGROUND
Mast cell tumors (MCTs) are the most common skin tumor in dogs and the second most common skin tumor in cats. Up to 14% dogs and 50% cats have multiple MCTs. In dogs, MCTs can have either a benign or malignant behaviour and this is largely dependent on histologic grade. Two histologic grading systems are now described: the older three grade system (where mitotic index is often used to determine prognosis for dogs with grade II MCTs) and the newer two grade system. Mast cell tumors contain granules which can release substances such as histamine, heparin, and prostaglandins. If MCTs degranulate, then a variety of conditions can occur such as hypotension (low blood pressure), gastric ulceration, and prolonged bleeding and delayed healing following biopsy. Mast cell tumors can metastasize to the lymph nodes or spread systemically similar to leukemia. Subcutaneous MCTs behave differently to cutaneous MCTs with lower local recurrence and metastatic rates. Nearly all cutaneous MCTs in cats are benign.
DIAGNOSIS
Mast cell tumors are diagnosed with fine-needle aspirates. Occasionally, an incisional biopsy is required for tumors in locations which are difficult to excise because determination of histologic grade will assist in surgical planning. Histologic grade cannot be determined from fine-needle aspirates.
CLINICAL STAGING
The incidence of lymph node metastasis is 25% for grade II MCTs and 49% for grade III MCTs. However, in one study of dogs with cutaneous MCTs, the sentinel lymph node (which is defined as the first draining lymph node) was different to the regional lymph node in 40% of dogs. For this reason, sentinel lymph node mapping and biopsy are recommended rather than excision of the regional lymph node. This involves peritumoral injection of a lipid-soluble contrast agent 24 hours prior to surgery (usually under sedation), regional radiographs immediately prior to surgery to identify the sentinel lymph node, and then peritumoral blue dye injection during surgery to aide in intraoperative identification and excision of the sentinel lymph node.



If there is a concern of a high-grade MCT, then other staging tests include abdominal ultrasonography, with ultrasound-guided aspirates of the liver and spleen, and bone marrow aspirates.
TREATMENT
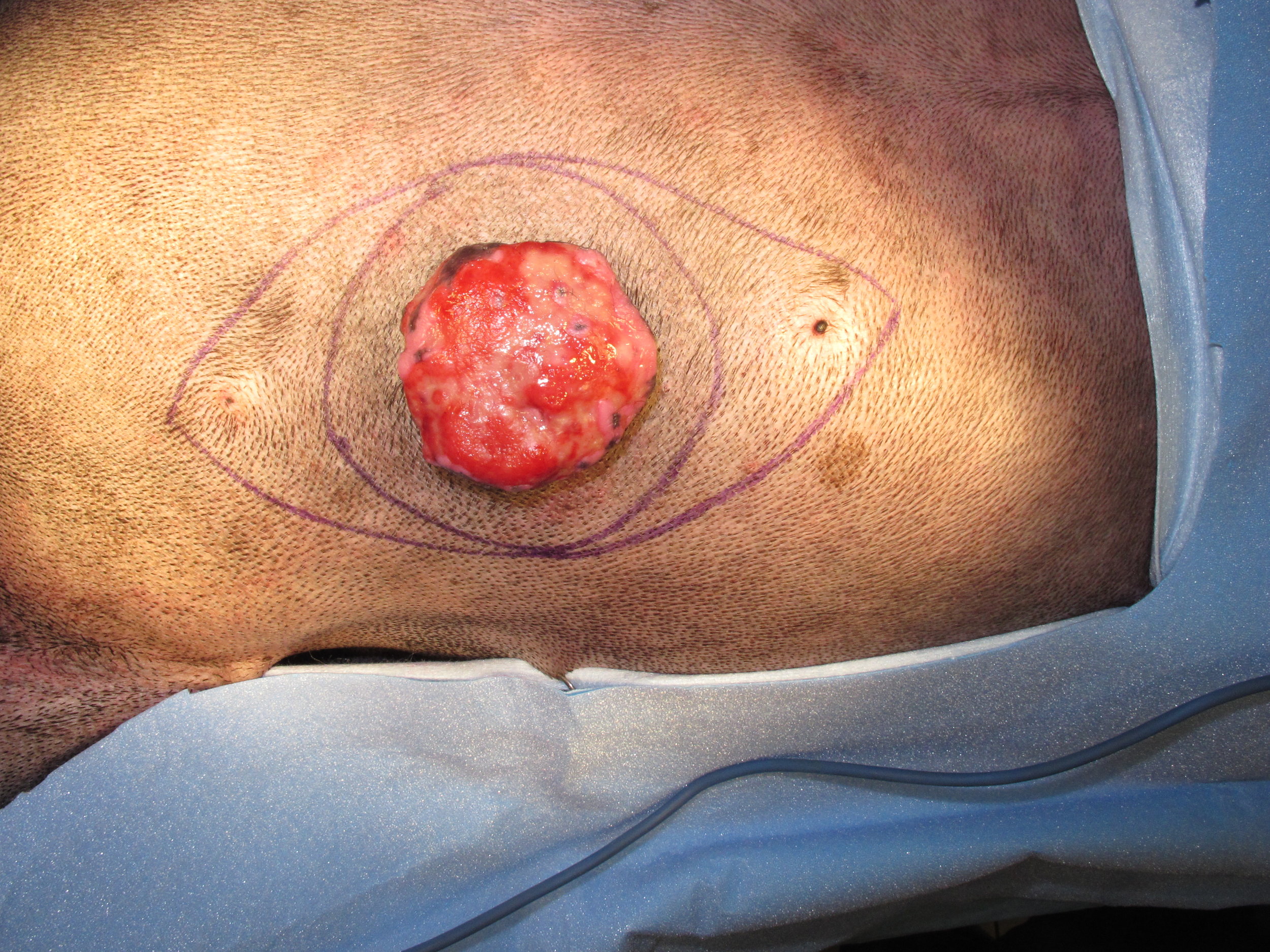
The recommended treatment for MCTs is surgical excision. In dogs, lateral margins for excisionn should either be 2cm or equal to the maximal diameter of the MCT, whichever is greater, and one fascial layer for deep margins. In difficult locations where there is limited skin available for closure, preoperative biopsy is recommended as only 1 cm margins are required for excision of grade I MCTs and 2 cm margins for grade II MCTs. Local tumor recurrence rates using this approach ranges from 0% to 11%.
Radiation therapy has been recommended for locoregional tumor control in dogs with stage II MCT disease (i.e., dogs with lymph node metastasis) and possibly for the management of dogs with incompletely excised MCTs. Other options for the management of incompletely excised MCTs include monitoring (although there is a significantly increased risk of tumor-related death in dogs with local recurrence); performing a MCT panel to evaluate whether there is an increased risk of local recurrence (using the combined Ki67 and PCNA scores) with further treatment recommended if this score is increased and monitoring if the score is not increased; performing a staging recut to evaluate if there is any residual MCT in the surgical scar with further treatment recommended if there is residual MCT and monitoring if there is no residual MCT; and wide excision of the surgical scar.
Chemotherapy is recommended for high-grade MCTs in dogs anhd dogs with stage II MCT (ie, lymph node metastasis). Chemotherapy drugs commonly used for the treatment of MCTs include vinblastine, prednisone, lomustine (or CCNU), and tyrosine kinase inhibitors such as Palladia.
PROGNOSIS
The prognosis is good to excellent for dogs with cutaneous MCT depending on their histologic grade and treatment.
Low-Grade Cutaneous Mast Cell Tumors
Grade I MCTs are often cured with surgical excision with 100% 2-year survival rates. Predicting the prognosis for grade II MCTs is difficult because some behave like grade I MCTs whereas others behave like grade III MCTs. Mitotic index can be used to differentiate grade II MCTs with a good or guarded prognosis. Dogs with low-grade II MCTs have a prognosis similar to grade I MCTs with a median survival time of 70 months.
High-Grade and Stage II Cutaneous Mast Cell Tumors
Dogs with high-grade II MCTs have a good prognosis when treated with a combination of therapies. The median survival time for dogs with high-grade MCTs treated with surgery alone is 4-6 months. However, median survival times are increased when surgery is combined with other therapies: 369 days when surgery is combined with chemotherapy (using mastinib); 1103 days when surgery is combined with chemotherapy (using vinblastine and CCNU) for dogs with stage II grade II MCTs; and 2056 days when surgery is combined with chemotherapy (using vinblastine and CCNU) and radiation therapy for dogs with stage II grade II MCTs. The prognosis for grade III MCTs is guarded with a 1-year survival rate of 24% following surgery alone (and a median survival time of 257 days), although the outcome is encouraging when surgery is combined with radiation therapy as the median survival time is 28 months with a 1-year survival rate of 71%.
Facial MCTs
The prognosis for dogs with MCTs in the oral cavity, perioral region, muzzle, and face is generally worse than for cutaneous MCTs in other regions. The metastatic rate to the regional lymph nodes (stage II) is higher for dogs with MCTs in this region (55%-72%) than non-facial regions. Prognostic factors for dogs with facial MCT include histologic grade and the presence of metastasis at the time of diagnosis. Overall median survival times range from 30-52 months following treatment with surgery and possibly radiation therapy and/or chemotherapy. Lymph node metastasis was prognostic in two studies: the median survival time for dogs with lymph node metastasis was 276-425 days while > 50% of dogs without lymph node metastasis were cured with surgery (and hence a median survival time was not reached). In one clinical study (2016), locoregional tumor control also had prognostic significance with a median survival time of 242 days when there was either residual MCT and/or metastatic lymph node, while the median survival time was not reached for dogs when the MCT (and metastatic lymph node if present) was completely excised or when incompletely excised MCT (and metastatic lymph node if present) were treated with postoperative radiation therapy. The 1- and 3-year local tumor control rates were 75% and 50%, respectively, in one paper.
Subcutaneous MCTs
The prognosis for dogs with subcutaneous MCTs is different and better than cutaneous MCTs. in a large series of 306 dogs, the local recurrence rate was only 8% (despite 56% being incompletely excised) and the metastatic rate was 4%. The median survival time in this study was not reached with estimated 1-, 2-, and 5-year survival rates of 93%, 92%, and 86%, respectively, with surgical excision alone. Poor prognostic factors included increased mitotic rate, infiltrative growth pattern, and presence of multinucleated giant cells.
Feline MCTs
The prognosis is excellent for cats with cutaneous MCT as the majority are cured with surgical excision, although local tumor recurrence is relatively common and reported in up to 24% cats.














Last updated on 6th March 2017